However, it might be mentioned here that without well-planned surveys, carried out in advance of the main body of medical opinion, the view that early diagnosis and treatment successfully improves the outlook for the condition in question is likely to become generally accepted. This in turn automatically renders unethical planned randomized trials of intervention by treatment, following early diagnosis; with the result that ideas about the effect of treatment pass into the realm of folklore rather than that of scientific knowledge.
The last sentence presciently sums up Breast Cancer Screening.
This article includes extensive quotations from screening guidelines, evidence documents, and my last article on “Rethinking Quality of Colon Cancer Screening.” I am choosing this style for the following reasons:
They are just too good NOT to publish.
They highlight the discrepancies in what is written in the guidelines and the contradictions with the recommendations.
To highlight data without my biases.
It made my life easier to write (put together) this article!
(Standard Disclaimer: The information below is NOT medical advice.)
The video version of this article is embedded below and available on my YouTube Channel.
The audio podcast and video versions are also available on the Podcasts Page.
Anatomy of Breast Cancer Screening Measure
Quality Measure Description
Percentage of women 50-74 years of age who had a mammogram to screen for breast cancer in the 27 months prior to the end of the Measurement Period
Denominator
Age 52-75 years of age
Numerator
Women who had one or more mammograms on or between October 1, two years before the measurement period, and the end of the measurement period.
What this complicated sentence means is:
If the measurement year is 2025, then
A mammogram should be done between October 1, 2023, and Dec 31, 2025.
Denominator Exclusions
History of Mastectomy
66 and older who meet criteria for BOTH Frailty AND advanced illness as defined by specific codes.
Billing codes (CPT and ICD-10) are still used in eCQM logic. As far as I know, most eCQMs allow for supplemental data, but how that will work in practice in the 2025 reporting year is up in the air.
Rationale for Quality Measure
The rationale for breast cancer screening is based on the 2024 USPSTF guidelines, which recommends screening individuals 40-74 years of age who are at average risk for breast cancer.1
Before we look at the data behind colorectal cancer screening, we need to define colorectal cancer. The standard definition of any cancer is “uncontrolled growth of cells,” but that raises the question, “At what point in the lifecycle do we decide that the growth is uncontrolled?”
The two lenses to define disease: natural history of progression of disease (backward-looking) and biologic pathway (forward-looking).
To make matters more complicated, we can look at this definition from two lenses:
Natural history of progression of disease (backward-looking): If we start with metastatic colon cancer that is causing symptoms, then we will attempt to define any polyp or dysplastic colon cells as either cancerous or pre-cancerous.
Biologic pathway (my preferred term and forward-looking): If we start with normal wear and tear of the colon wall, which leads to the production (and destruction) of dysplastic cells and even polyps, then the definition becomes a lot harder.
Is very polyp going to spread and/or cause symptoms? If they spread, how long will it take the polyp to spread—months, years, or decades?
What level of dysplasia needs to be present to define pre-cancer?
What level of spread should be present to define colon cancer?
How we define colorectal cancer will determine its incidence rate and 5-year survival rates due to lead time bias. In other words, if we define cancer earlier in the pathway, screening tests will appear to save lives!
This also applies to breast cancer.
In addition, recently, we added Ductal Carcinoma in Situ (DCIS) as a “cancer diagnosis” (more on DCIS under the overdiagnosis section below).
A Mini-Critical Look at USPSTF Guidelines
USPSTF gives breast cancer screening a Grade B recommendation based on available data.
USPSTF’s decision to grant a Grade B recommendation is based on the Evidence Synthesis document published in 2016 (PDF Link). Per the guidelines, the Relative risk (RR) reductions in breast cancer mortality are:
0.88 (95% CI, 0.73-1.003; 9 trials) for women aged 39 to 49 years (i.e., not statistcally significant)
0.86 (95% CI, 0.68-0.97; 7 trials) for women aged 50 to 59 years
0.67 (95% CI, 0.54-0.83; 5 trials) for women aged 60 to 69 years
0.80 (95% CI, 0.51-1.28; 3 trials) for women aged 70 to 74 years (i.e., not statistcally significant)
An updated analysis of 3 Swedish screening trials reported a 15% relative reduction in breast cancer mortality for women aged 40 to 74 years (RR, 0.85 [95% CI, 0.73-0.98]).2
None of the trials nor the combined meta-analysis demonstrated a difference in all-cause mortality with screening mammography.
Now let’s look at what the 2016 synthesis document has to say about the trials that were included that led to Grade B recommendation:
No trials met the criteria for good quality (all RCTs in the meta-analysis were fair-quality; a poor-quality trial was excluded).
…
The applicability of the screening trials to current populations and practice has likely decreased over time. All of the trials were conducted in the past when imaging technologies and breast cancer therapies were markedly different than today.
…
In general, women who enroll in trials and attend screening interventions differ from those who do not … women at higher risk of breast cancer but lower risk of all-cause mortality may choose to participate in screening. These are important differences that could influence outcomes.
And:
None of the RCTs were designed to evaluate screening intervals.
Two trials conducted in the 1980s to 1990s reported no difference in breast cancer mortality or breast cancer features such as tumor size, node positivity status, or histologic grade when comparing annual vs triennial screening.
In summary:
Relative Risk Reduction (RRR) in the guidelines is NOT based on high-quality RCTs (they are fair to low-quality RCTs).
Yearly vs. every 2 years interval for screening is based on data modeling (existing non-randomized trials compare yearly vs. every 3 years screening).
Digital mammograms used today are more sensitive than the film-based mammograms used in the original studies—and are more sensitive.
Given the higher sensitivity of digital mammograms, the real-life false positive rate is much higher than published data (11%—19%).
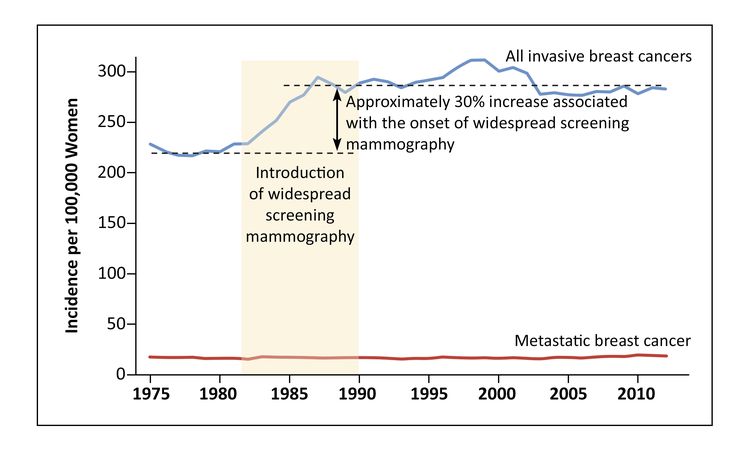
Cancer.gov has an excellent article with a graph showing a 33% increase in false positive rates after implementing mammography. This graph also shows that there was no change in the rate of metastatic breast cancer. Unfortunately, I cannot reproduce the graph here due to copyright issues, but this is a direct image link.
Furthermore, there is NO data to support the use of breast ultrasound or MRI for screening.
The USPSTF found no studies of supplemental screening with MRI or ultrasonography, or studies of personalized (eg, risk-based) screening strategies, that reported on morbidity or mortality or on cancer detection and characteristics over multiple rounds of screening.
And, if this was not enough, the decision to lower the age from 50 to 40 is based on data modeling, even though the (old) RCTs did not show any benefit. A NEJM Perspective article published a brutal takedown of USPSTF’s decision to lower the age of mammography screening from 50 to 40 years.3
(For people interested in an in-depth review, I recommend this YouTube Video.)
One may criticize the above data as being too focused on USPSTF guidelines while ignoring data from other societies. While there is merit to the argument, my counterargument would be:
Most societies use the same/similar data but draw either identical or different conclusions.
This is why I published quotes from the original articles so that people can make their own decisions.
The quality measures are based on USPSTF guidelines!
Talking about other guidelines, let us take a look at the recommendation by ACOG (American College of Gynecology), especially since gynecologists also order a lot of mammograms:
Women at average risk of breast cancer should have screening mammography every 1 or 2 years based on an informed, shared decision-making process that includes a discussion of the benefits and harms of annual and biennial screening and incorporates patient values and preferences.
In practice, at least in my neck of the woods, most women end up getting mammograms yearly!
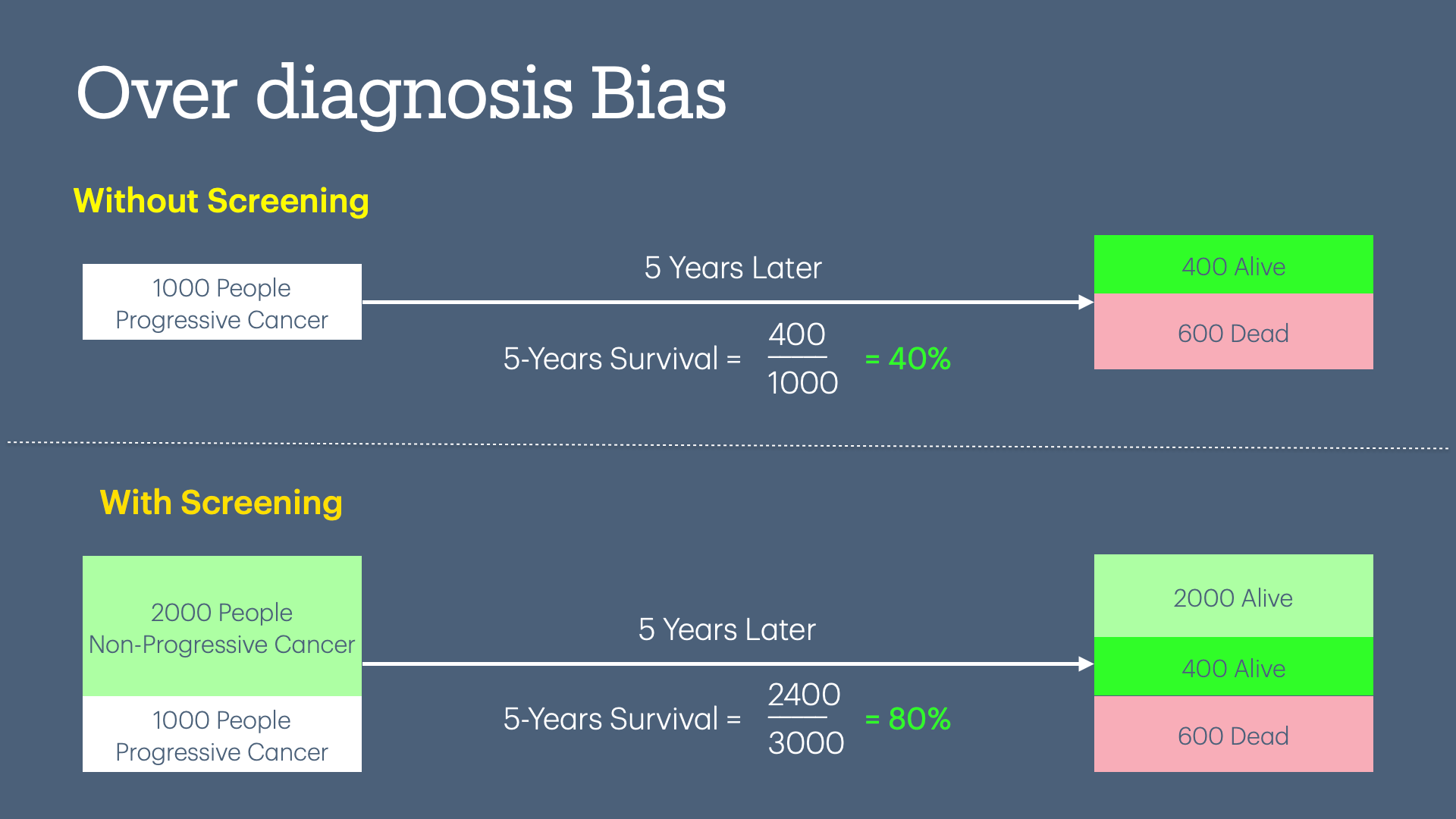
There are statistical techniques that can give the appearance of efficacy to a test when, in fact, the test is completely useless.
These techniques include over-diagnosis bias, lead time bias, and length time bias. For an overview of these techniques, please see my previous article (I promise it is not technical or math-heavy). All of these statistical techniques apply to breast cancer screening studies.
Overdiagnosis
Overdiagnosis occurs when breast cancer that would never have become a threat to a person's health, or even be apparent during their lifetime, is found due to screening.
Between 20% and 50% of screen-detected cancers represent overdiagnosis based on patient age, life expectancy, and tumor type (ductal carcinoma in situ and/or invasive).4
Regarding DCIS, per USPSTF guidelines:
Ductal carcinoma in situ (DCIS) is a noninvasive condition with abnormal cells in the breast duct lining with uncertainty regarding its prognostic significance. Consequently, there is clinical variability in the treatment approach when DCIS is identified at screening. It is unknown what proportion of screen-detected DCIS represents overdiagnosis.
And per ACOG:
Reported rates of overdiagnosis and overtreatment are, in part, related to the management of ductal carcinoma in situ. This lesion has a significantly lower risk than breast cancer, although many studies group it with breast cancer and its diagnosis typically leads to treatment.
False Positives
The difference between over-diagnosis and false positives is:
Over-diagnosis: after additional workup, the person is diagnosed with breast cancer, but there is no improvement in life expectancy.
False positive: after additional workup, the person is not given a diagnosis of breast cancer.
Per ACOG, the 10-year, cumulative false-positive rate of:
61% with annual screening
7% biopsy rate
42% with biennial screening
5% biopsy rate
Dense breasts were associated with an increased likelihood of false-positive test results among women aged 40–49 years.
Also, once a biopsy is done, the chance of a false positive rate increases in subsequent mammograms, and possibly increases the risk of breast cancer itself.5
Furthermore, the most significant harm of false positives is the increase in anxiety and distress, which may, in turn, lead to further unnecessary testing.
Radiation Exposure
Screening mammography uses ionizing radiation, a known carcinogen. While the radiation dose in each exam is minimal, exposure is cumulative.6
The number of deaths due to radiation induced cancer from screening with digital mammography was estimated through modeling as between 2 to 11 per 100,000 depending on age at onset and screening intervals.
Resource Allocation & Access to Care
Radiologists are limited in availability, and the time spent interpreting screening mammograms could be better utilized for reviewing imaging studies of symptomatic patients. How often have hospital discharges been delayed due to pending radiology results?
At the Intersection of Assumption, Advertising & Quality
Many people are unaware of the true risks and benefits of colon cancer screening and often believe it unequivocally saves lives. Aggressive advertising from large health organizations reinforces this misconception. This is further compounded by making colon cancer screening a quality measure, which disincentivizes doctors to fully inform patients about the potential risks of screening—as patients who decline colon cancer screening will negatively impact the physician's performance metrics, penalize them in value-based contracts and increase their malpractice risk.
This is truer for breast cancer screening—just google mammogram parties! (my goal here is not to make fun of mammogram parties but to highlight the aggressive advertising by health systems).
Here is the 2025 Superbowl ad for breast cancer screening by Novartis, which just got approval for Kiskali, a breast cancer chemotherapy medication.
Improving Performance on Breast Cancer Screening Quality Measure
CPT-I and ICD-10 Codes
Insurance plans credit PCPs/ACOs for breast screening quality measures based on the CPT/ICD-10 codes submitted by radiology when a mammogram is performed.
Doctors (PCP, Oncologist, or surgeon) must bill using appropriate CPT and ICD-10 codes during an office visit in the measurement year to qualify the patient for denominator exclusions (e.g., diagnosis of breast cancer, mastectomy, etc).
CPT-II Codes
There is 1 CPT II code for breast cancer screening. Once CMS switches to eCQM, this will not be accepted.
3014F: Screening mammography results documented and reviewed.
Supplemental Data Submission
This involves manually collecting mammography reports and submitting them to insurance companies.
Also, manual collection and submission of denominator exceptions is a big mess, with every plan creating its own rules on what it will/will not accept.
Artificial Intelligence can help find and collate the supplemental data for submission to the insurance company. However, this benefits larger organizations with a single EHR at the expense of small PCP practices.
Conclusion
Given the data, the best conclusion is that we have no idea how many (if any) people will benefit from screening mammography, with a small but unknown percentage of harm. Most modeling studies, such as using the CISNET database (including the decision to lower the screening age to 40), are based on our assumptions and biases that we feed into the models—no wonder all the models show that mammography saves lives!
Since there is a huge demand and almost religious belief in mammography, we badly need new trials to assess the efficacy of mammograms for breast cancer screening. While we wait for the new trials, ACOG has the best recommendation for breast cancer screening:
Shared decision making is particularly important for decisions regarding breast cancer screening because many choices involve personal preferences related to potential benefits and adverse consequences.
Making breast cancer screening a quality measure is an excellent way to undermine shared decision-making and informed consent.
Up Next
In the next article, I will look at the “Controlling Blood Pressure” quality measure—it serves as a great political slogan but is absolutely bonkers in how it is measured.
US Preventive Services Task Force. (2024). Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA, 331(22), 1918–1930. https://doi.org/10.1001/jama.2024.5534
Nyström, L., Bjurstam, N., Jonsson, H., Zackrisson, S., & Frisell, J. (2017). Reduced breast cancer mortality after 20+ years of follow-up in the Swedish randomized controlled mammography trials in Malmö, Stockholm, and Göteborg. Journal of Medical Screening, 24(1), 34–42. https://doi.org/10.1177/0969141316648987
Woloshin, S., Jørgensen, K. J., Hwang, S., & Welch, H. G. (2023). The New USPSTF Mammography Recommendations—A Dissenting View. New England Journal of Medicine, 389(12), 1061–1064. https://doi.org/10.1056/NEJMp2307229
Visscher, D. W., Frank, R. D., Carter, J. M., Vierkant, R. A., Winham, S. J., Heinzen, E. P., Broderick, B. T., Denison, L. A., Allers, T. M., Johnson, J. L., Frost, M. H., Hartmann, L. C., Degnim, A. C., & Radisky, D. C. (2017). Breast Cancer Risk and Progressive Histology in Serial Benign Biopsies. JNCI Journal of the National Cancer Institute, 109(10), djx035. https://doi.org/10.1093/jnci/djx035
Miglioretti, D. L., Lange, J., van den Broek, J. J., Lee, C. I., van Ravesteyn, N. T., Ritley, D., Kerlikowske, K., Fenton, J. J., Melnikow, J., de Koning, H. J., & Hubbard, R. A. (2016). Radiation-Induced Breast Cancer Incidence and Mortality from Digital Mammography Screening: A Modeling Study. Annals of Internal Medicine, 164(4), 205–214. https://doi.org/10.7326/M15-1241




{kind=link}